
Content verified by

Hirschsprung disease in children, sometimes called congenital megacolon, is a rare congenital (from birth) condition. It affects around 1 in 5,000 babies and is 3 to 4 times more common in boys than girls.
At Guy’s and St Thomas’ Specialist Care, our paediatric surgeons are committed to providing treatment, care and support for children with Hirschsprung disease.
What is Hirschsprung disease in children?
Hirschsprung disease affects the function of your child’s colon, making it challenging for them to empty their bowels (poo).
During digestion, nerve cells called ganglion cells send signals to the muscles in the colon to tense and relax, in order to move waste (poo) through the intestines. This waste ends up in the rectum, activating nerves in the anus to feel the need to poo.
In Hirschsprung disease, the nerve cells near the end of your baby’s large intestine haven’t developed as they should. This means that when poo reaches the final portion of the colon, it moves slowly or stops, making it difficult for your baby to poo.
In rare cases, Hirschsprung disease can affect the entire large intestine (long-segment disease), but more commonly, it affects a shorter colon length closer to the rectum (short-segment disease). Short-segment disease is more common because an unborn baby’s cells first develop from the top of the intestine and fail to reach the lower part of colon and rectum.
Hirschsprung disease, if left untreated, can lead to severe constipation and blockage of bowel, swelling of tummy and green (bile stained) vomiting, and sometimes enterocolitis, a serious bowel infection.
What are the signs and symptoms of Hirschsprung disease in children?
The symptoms of Hirschsprung disease can vary depending on its severity and how much of the intestine is affected.
In severe cases, a baby usually shows symptoms within the first few days of life. Some babies with Hirschsprung disease have blocked intestines at birth.
Your baby may have Hirschsprung disease if they haven’t pooed within 48 hours after birth.
Signs of Hirschsprung disease in a newborn include:
- not passing meconium (dark, tar-like poo) within 48 hours
- a swollen belly, bloating or gas
- green (bile stained), yellow-green or brown vomit
Doctors might not spot the less severe cases of Hirschsprung disease until a child is a little older.
The signs of Hirschsprung disease to look for in infants and older children include:
- swollen belly
- constipation
- trouble gaining weight
- vomiting (green, bile stained)
- failure to pass gas or poo through back passage
- loss of appetite
- delayed growth
What causes Hirschsprung disease in children?
A series of contractions called peristalsis are responsible for moving digested material through the gut and out of the body as poo. Nerves between the layers of muscle tissue in the intestine control peristalsis.
In Hirschsprung disease, these crucial nerves are missing in some parts of the intestine, which prevents it from relaxing, causing a spasm of the affected bowel, blockage of waste, and difficulty pooing.
We don’t yet understand why these nerves are absent in some babies, but we know that Hirschsprung disease can run in families. Children with Down’s syndrome and genetic heart conditions are also at an increased risk of having Hirschsprung disease.
Diagnosing Hirschsprung disease in children
Hirschsprung disease is usually diagnosed soon after birth, typically in the first 4 weeks of life.
If your baby or child shows signs of Hirschsprung disease, your doctor will likely perform one or more tests to confirm a diagnosis.
Newborns may need the following tests:
- physical examination of the abdomen (tummy)
- rectal examination and biopsy (taking a small tissue from lining of back passage) – a doctor or nurse will gently insert a finger into your baby’s rectum to feel for abnormalities
- abdominal X-ray – to show any blockages or bulges in the bowel, which indicate Hirschsprung disease
- rectal biopsy – a doctor will insert a small instrument the size of a pen into your child’s rectum to take a sample of tissue to examine for ganglion cells (the biopsy is taken from an area of the rectum, which has touch sensation and it is painless)
- contrast enema – a small tube called a catheter is inserted into your child’s rectum to fill their large intestine with a special dye that highlights any blockages or intestinal narrowing on a special X-ray which also helps to treat the blockage
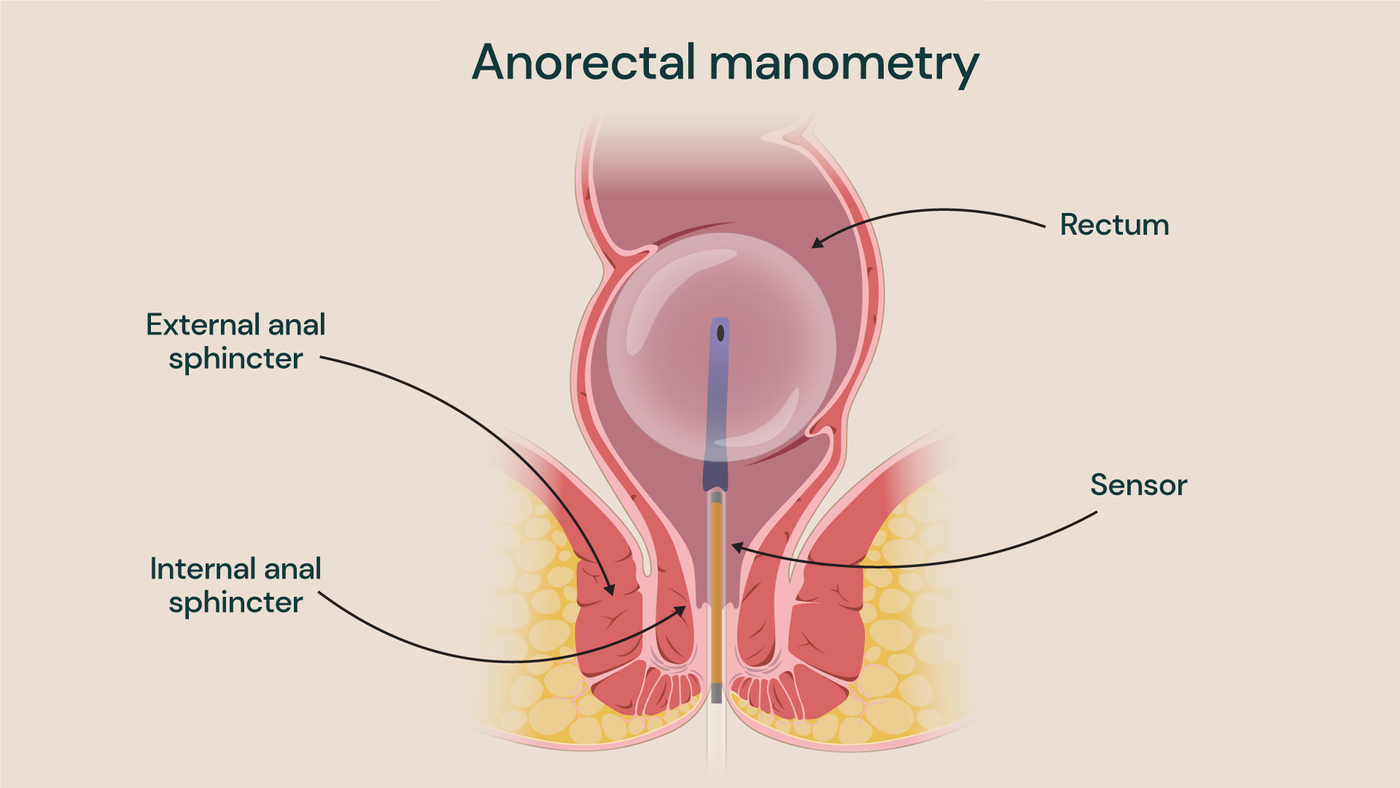
- anorectal manometry – typically only used to diagnose Hirschsprung disease in older children. The test involves inserting a small balloon into the rectum to record pressure changes and assess the anal sphincter’s function (the ring of muscles that controls the anal canal) and relaxation of the sphincter in response to inflating the rectal balloon
Treating Hirschsprung disease in children
All children with Hirschsprung disease need surgery to treat the condition.
There are 2 types of surgery to treat Hirschsprung disease: pull-through surgery and a temporary ostomy to relieve the bowel blockage. A temporary ostomy is recommended if initial treatment with rectal washouts (passing a small tube through the back passage to irrigate the colon) is not successful. The type of surgery your child needs will depend on the severity of their condition.
In most cases, babies or children will undergo pull-through surgery, usually at around 3 to 4 months of age. During this time, parents are trained to perform daily rectal washouts at home. This helps reduce the swelling in the large intestine, making the surgery safer and reducing the need for a stoma in the future.
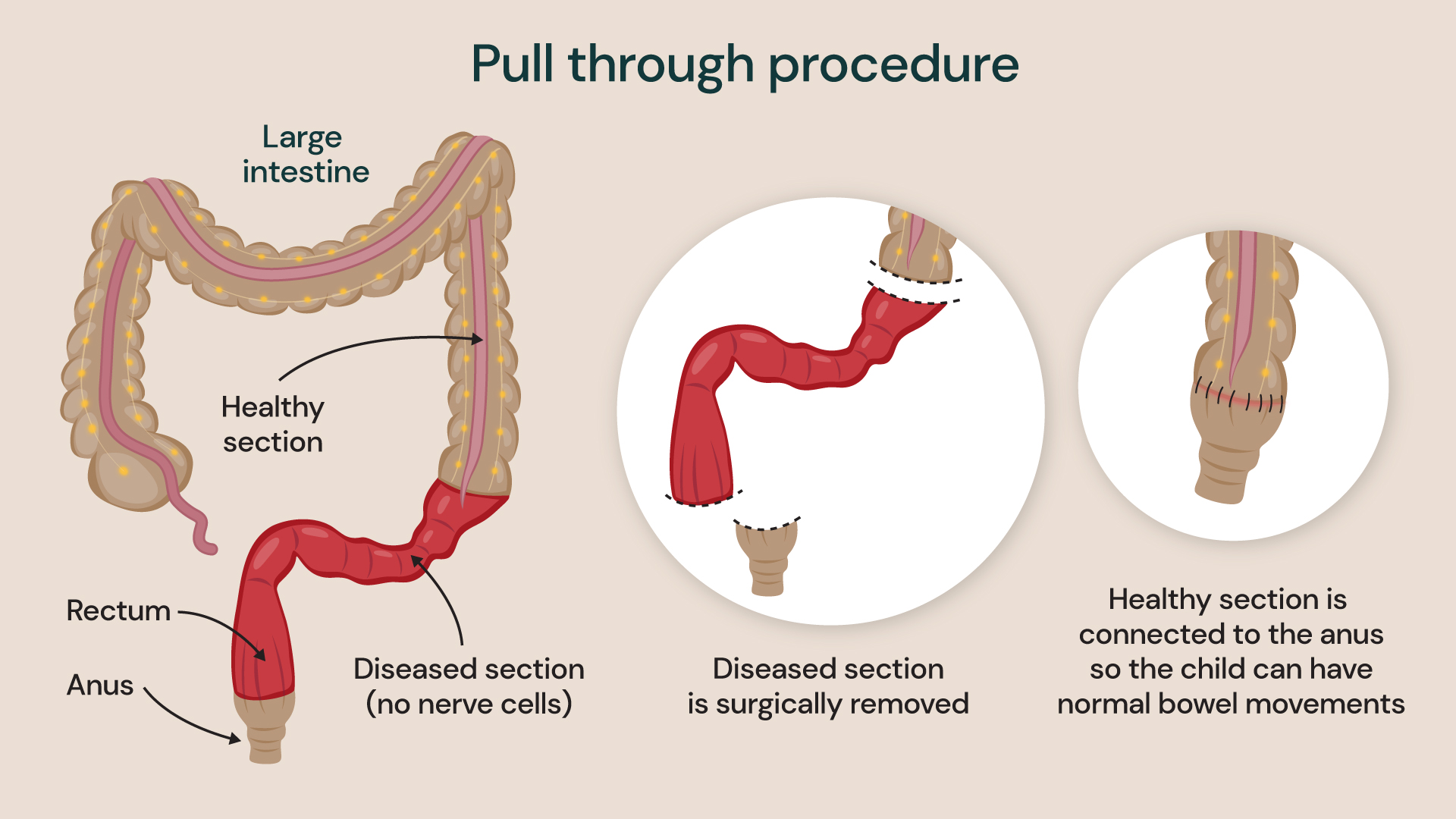
During the procedure, the surgeon removes the section of the large intestine that is missing nerve cells and connects the healthy part of the intestine to the anus. The surgery can be performed either laparoscopically (keyhole surgery) or as an open procedure, which involves making a larger cut in the child’s tummy.
Your child may need a procedure called ostomy surgery if they’re not well enough for pull-through surgery, or if they fail to pass bowel motion with the rectal wash out. Instead of cutting out the affected section of the intestine, your child’s surgeon will divert their bowel through a temporary opening in their tummy called a stoma.
The child’s poo will come out of this opening and collect in a pouch until they are well enough to undergo pull-through surgery. During pull-through surgery, the surgeon will remove the affected bowel section and join the healthy section to the anus. The opening in the tummy may be closed at the same time or a few weeks later in a follow-up procedure.
Your child must stay in the hospital for a few days after surgery for observation, and we’ll give them pain relief to help them feel more comfortable. We’ll also give them fluids via a vein until they can tolerate eating and drinking.
Surgery is an effective treatment for most children but, as with any procedure, some risks are involved.
Risks of surgery for Hirschsprung disease
Rare complications of surgery for Hirschsprung disease in children include:
- bleeding during or after surgery
- infection of the bowel (enterocolitis)
- serious infection caused by leaking of the bowel content where it joins the back passage (peritonitis)
- narrowing or blockage of the bowel at the site of join, requiring further surgery
- the need for a permanent stoma (in very rare cases)
Most children have well-functioning bowels and can poo normally after surgery, although some may take a bit longer to toilet train or require laxative treatment.
Some children may experience persistent constipation or have trouble controlling their bowels (bowel incontinence) after toilet training. In this case, your doctor can offer advice and further treatment if needed.
Before and after treatment for Hirschsprung disease in children
Your specialist will advise whether your child should stay in the hospital or if you can look after them at home while they wait for surgery. They will also provide you with any preparation steps you need to follow to ensure that your child is ready for surgery.
Following their operation, your baby or child may need to:
- receive fluids directly into a vein instead of being milk-fed
- have a tube through their nose and into their stomach to drain, collecting fluid and air
- take antibiotics to prevent infection
If you have any questions, do not hesitate to contact us.
Locations
Our specialists offer treatment for Hirschsprung disease in children at the following locations:
Explore our team of gastrointestinal surgeons
Meet our paediatric gastrointestinal surgeons. Our specialists provide access to the breadth of clinical services, ensuring high quality, expertise and personalised care for our patients.